


Primary Frozen Shoulder occurs in approximately 2-5.3% of the general population!
Secondary Frozen Shoulder is associated with Diabetes Mellitus and Thyroid Disease (Hypothyroidism) ~ 4.3 - 38% of individuals!
Anatomy
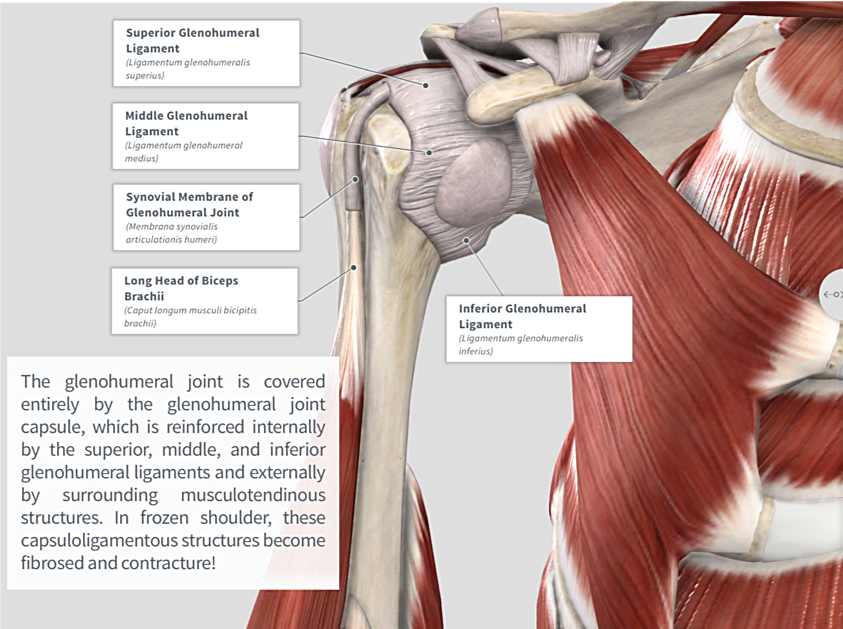
Image via Complete Anatomy 2018 by 3D4 Medical
Key Findings

Aside from clinical findings in the subjective exam, patients with adhesive capsulitis will also present with impaired glenohumeral joint range of motion actively and passively (depending on the stage). This restriction typically follows the capsular pattern of the glenohumeral joint: external rotation, abduction, and internal rotation going from most restricted to least restricted. Flexion also tends to be limited and is often accompanied by compensatory shoulder girdle elevation. (Click image to watch 1-2 minute video)
Treatment & Therapeutic Exercise

Treatment depends on stage and irritability of the patient. If the patient has low to moderate irritability and demonstrates capsular restriction, research shows that posterior and inferior glides may be beneficial toward improving pain and range of motion in these individuals! (Click image to watch 1-2 minute video)

Research demonstrates moderate evidence to support the use of stretching exercises in individuals with adhesive capsulitis. Exercises should be matched to patient tolerance; if open chain proves to be too difficult, light closed chain range of motion exercises may be a better choice! (Click image to watch 1-2 minute video)
*Clinical Side Note: When working with individuals with adhesive capsulitis it is important to remember that the process could last 12-18 months with symptoms potentially being present longer. Education on the process and managing patient expectations is an integral part of the rehabilitation process. Depending on the stage of adhesive capsulitis, as well as clinical judgement, it may be beneficial to postpone use of patient visits until progress can be made!